Our approach to Peyronie’s Disease surgery is to first determine that the disease is stable (no change in curvature for 6 months) and that the erectile function is good. We then discuss all options. Surgery is generally the most effective option to straighten the penis.
The curvature correction options are Peyronie’s disease graft surgery or Peyronie’s disease plication surgery. We offer both options, and carefully counsel patients before surgery. It is not uncommon for men to contact us requesting a particular Peyronie’s surgery, but many of these men are not aware of all of the risks and benefits of each option. This understanding should come before decision making.
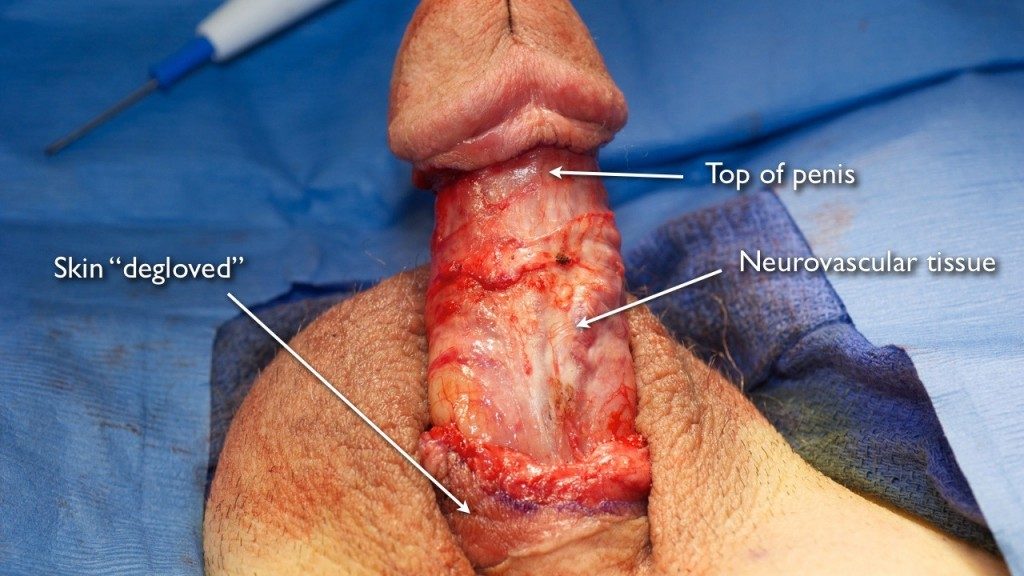
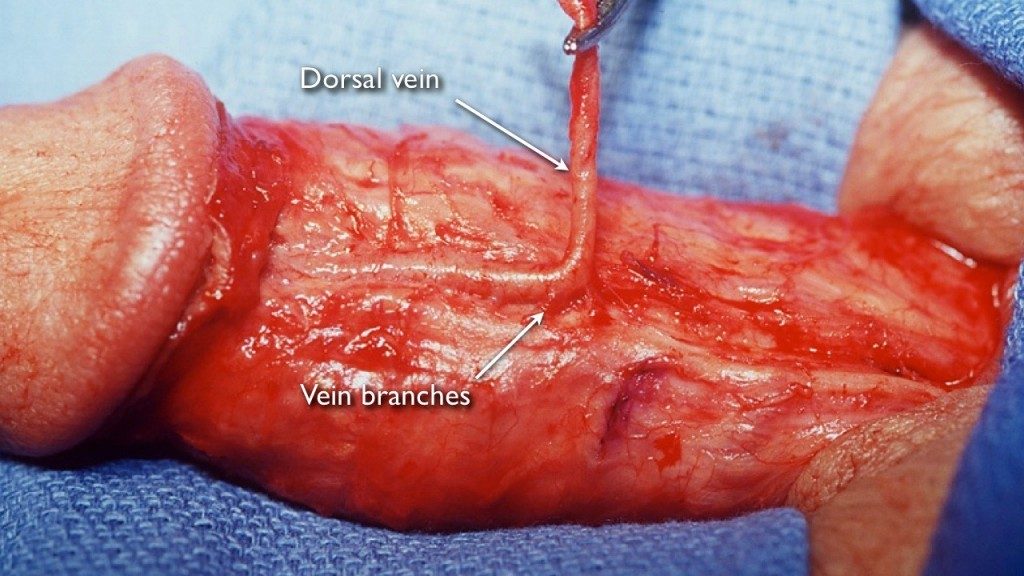
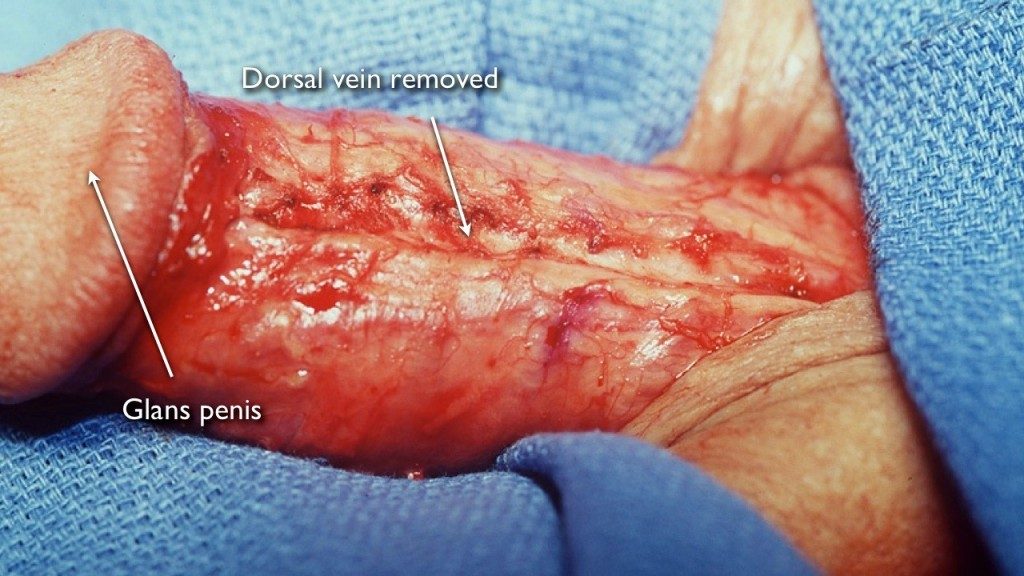
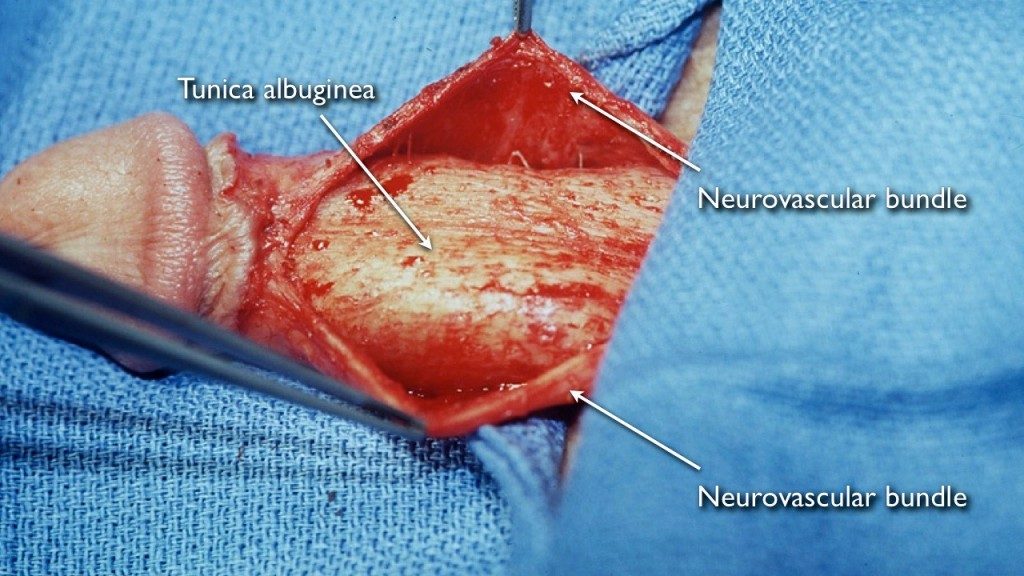
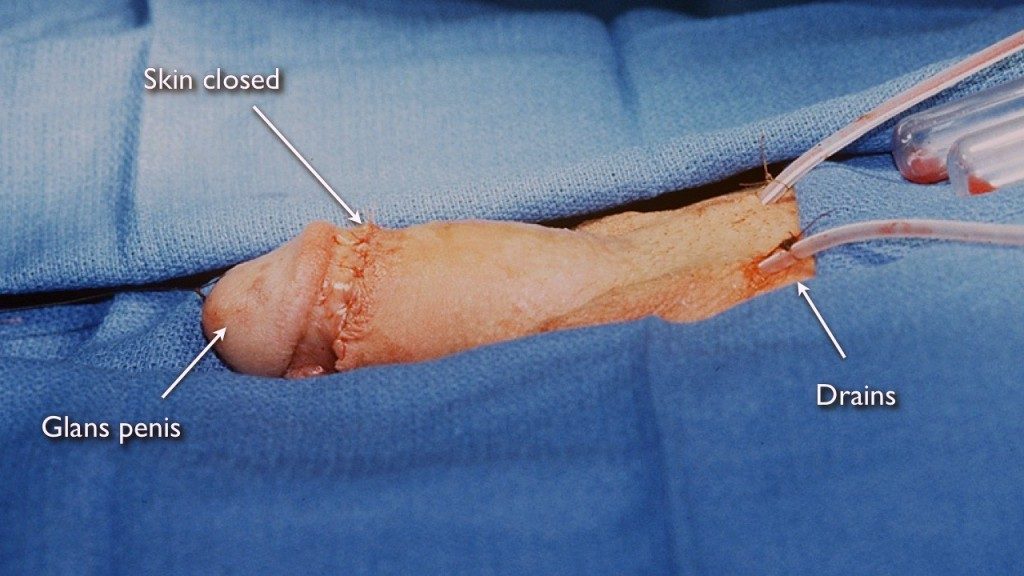
Below we detail our surgical approach and the Peyronie’s disease surgery results for both methods. These are slideshows depicting actual surgery with graphic pictures demonstrating how we fix penile curvature with before and after photographs.
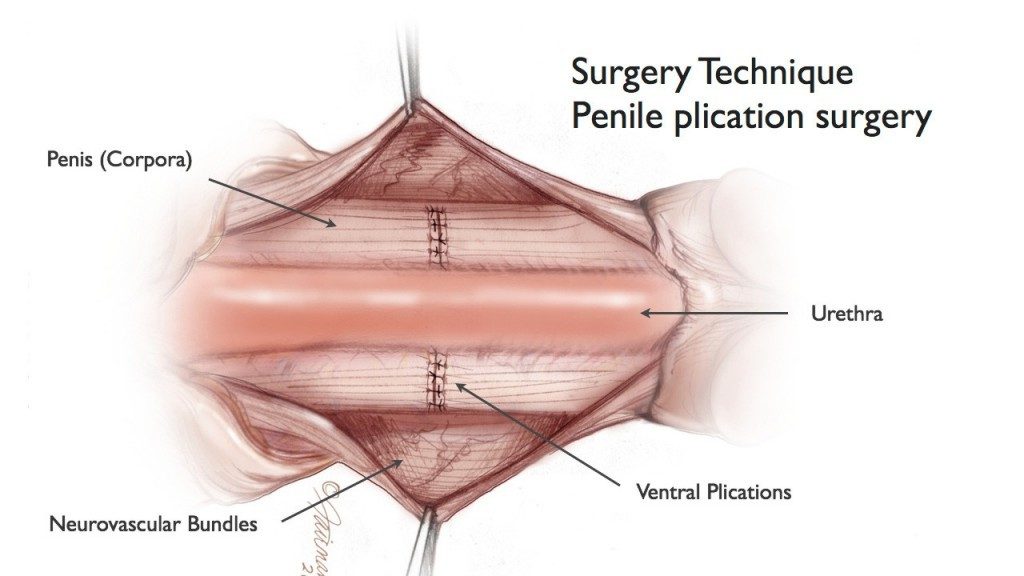
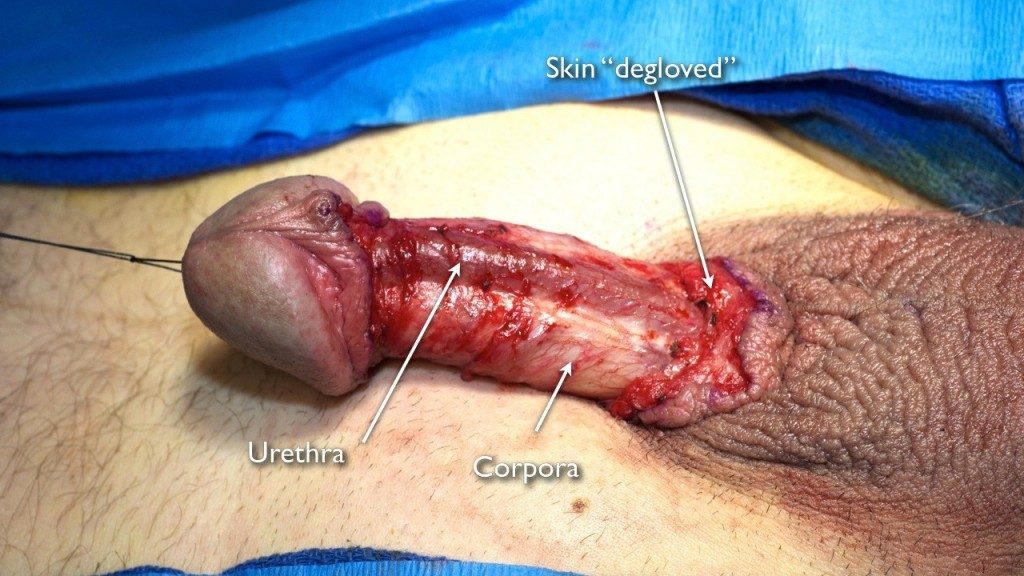
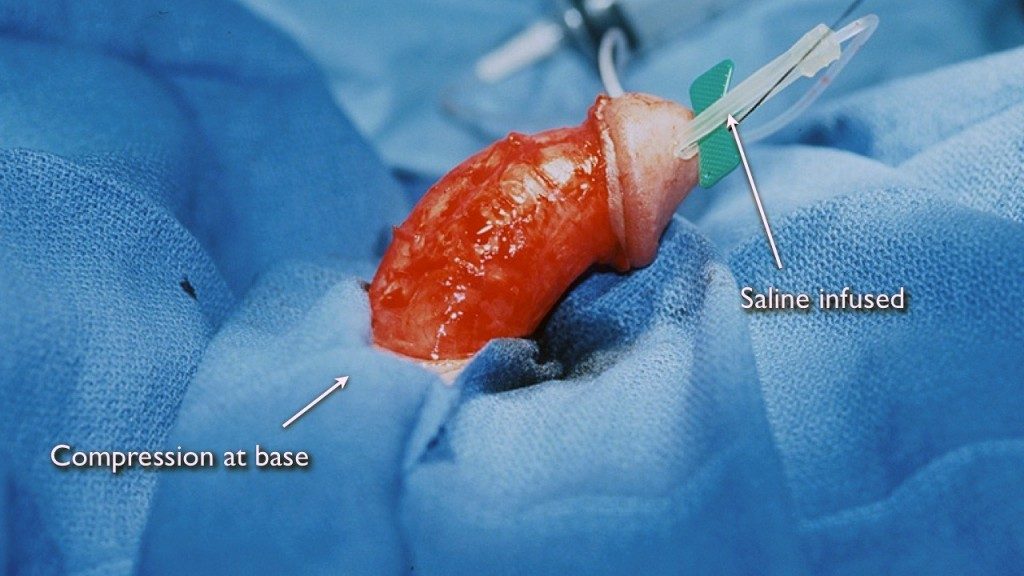
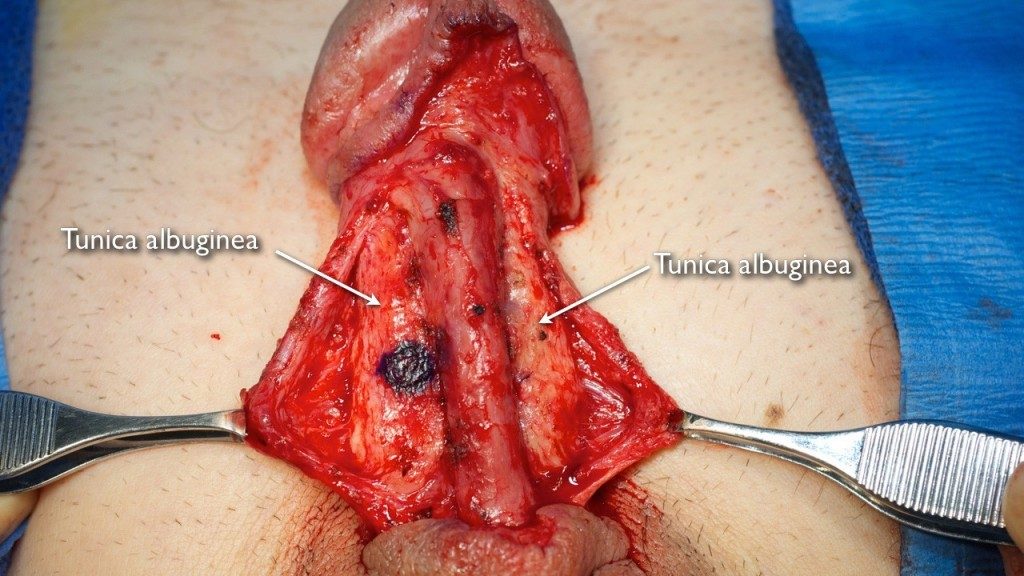
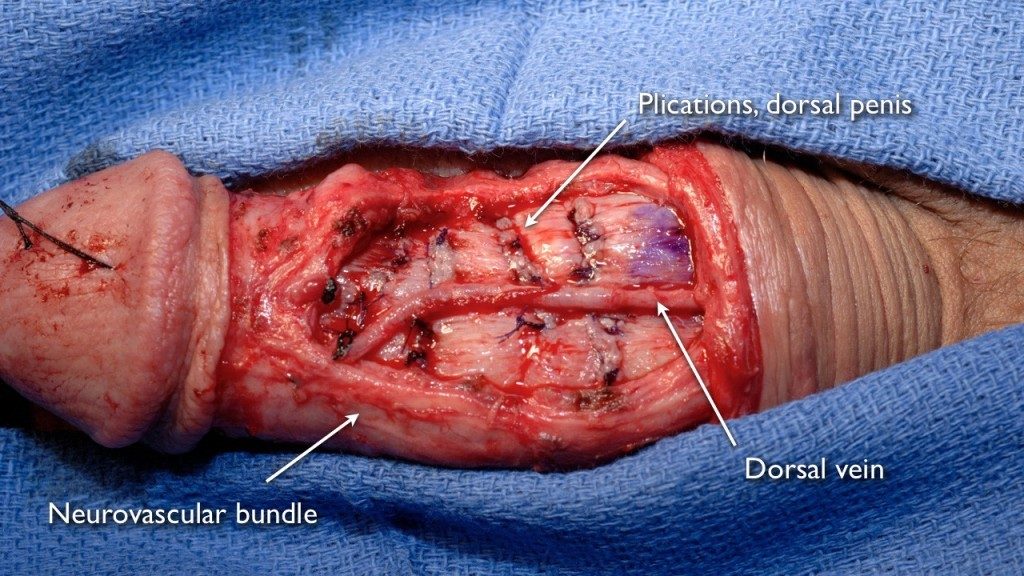
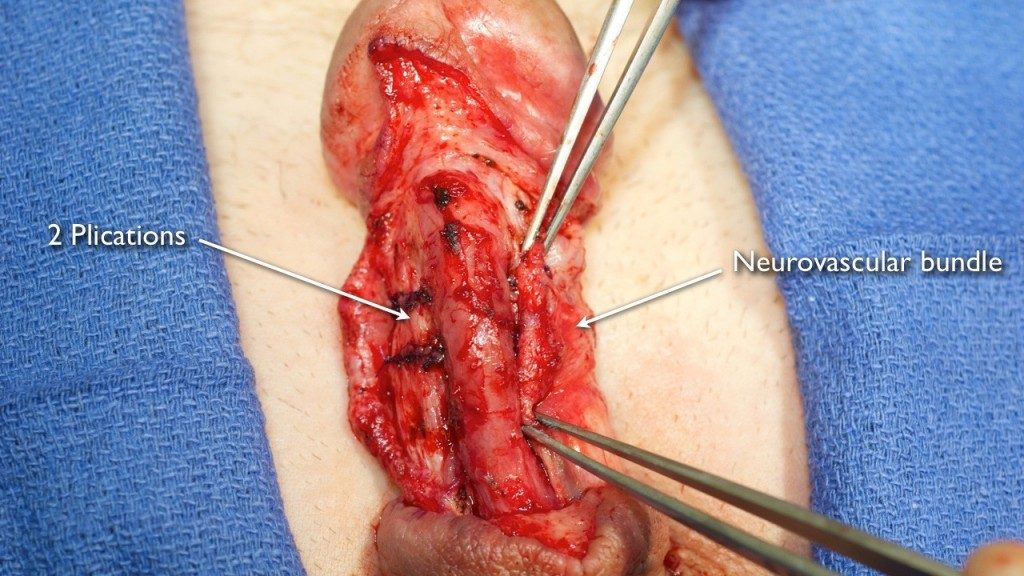
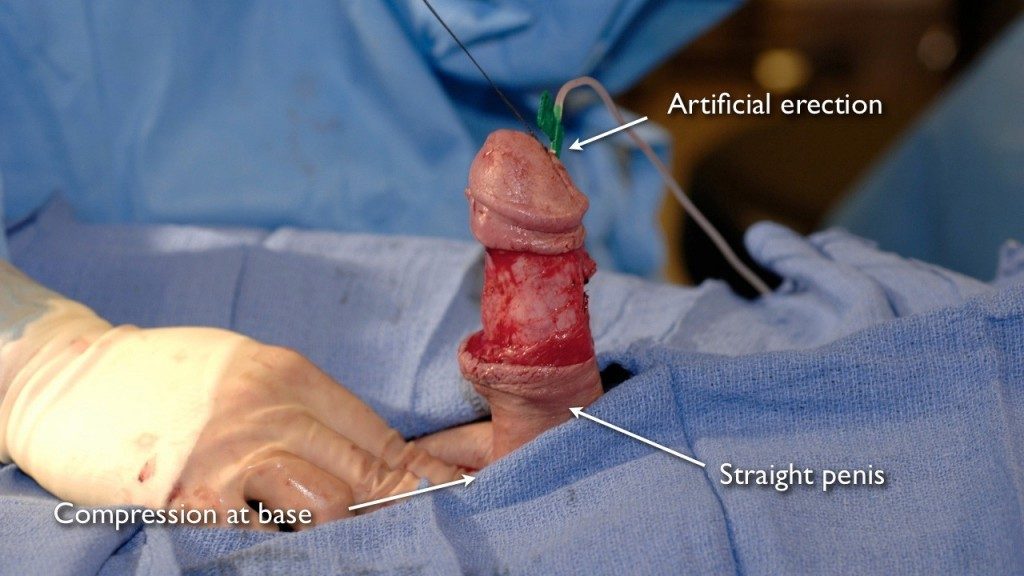
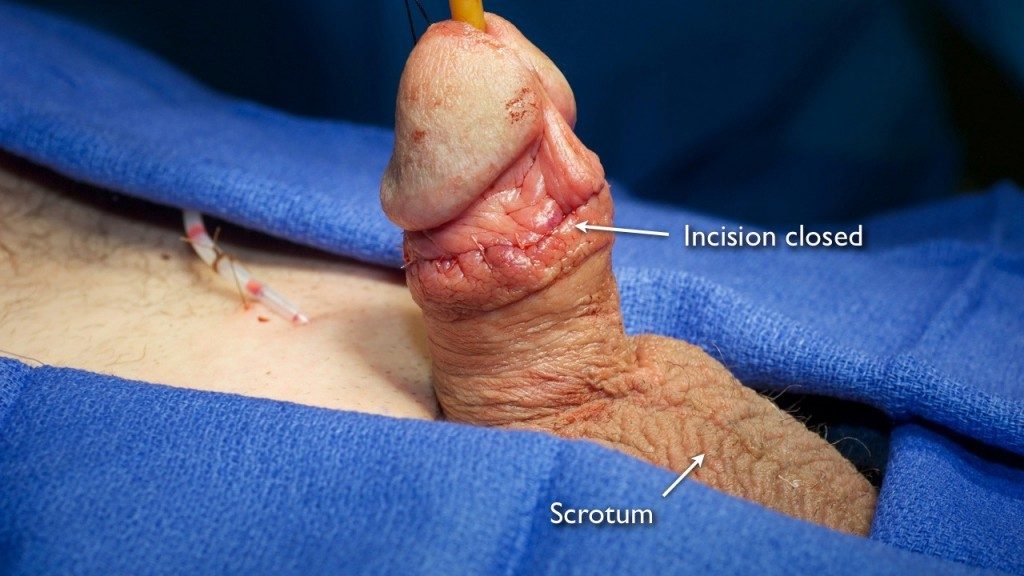
Peyronie’s Disease Plication Surgery
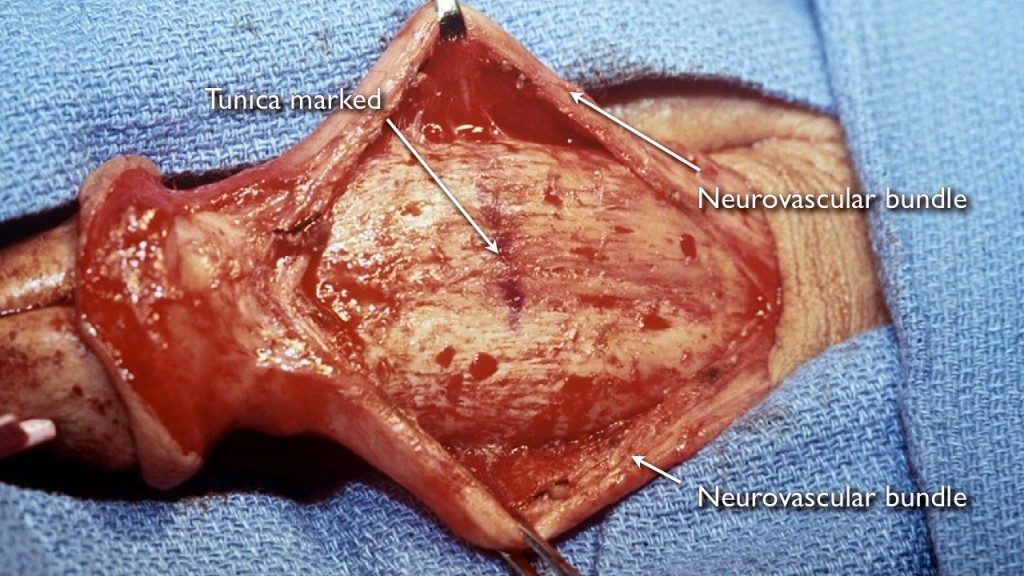
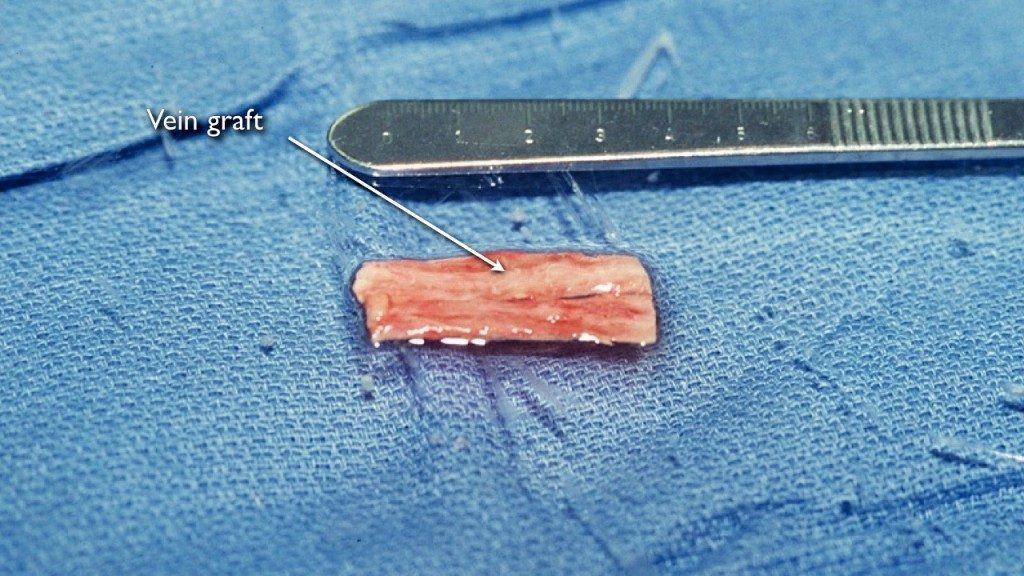
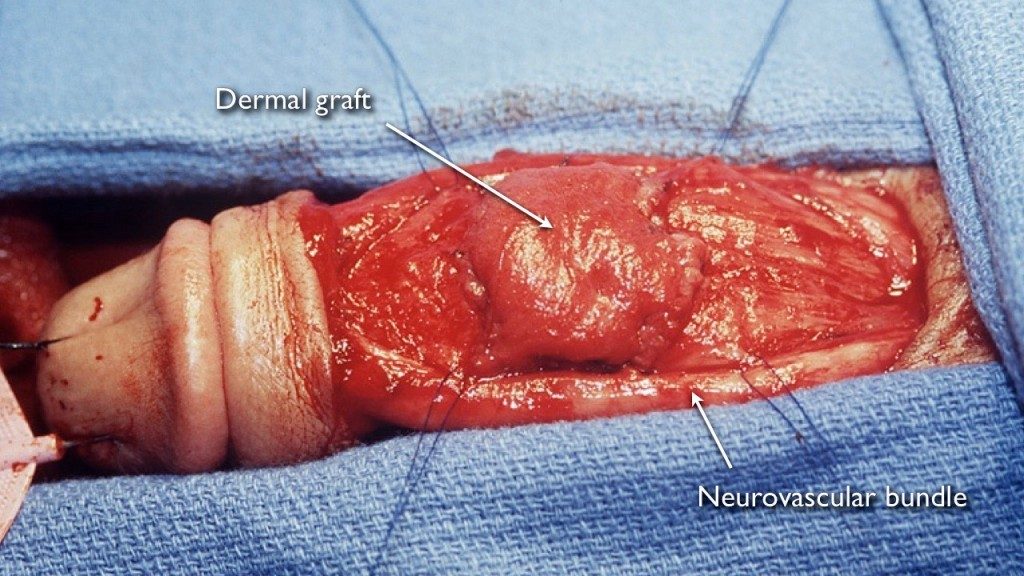
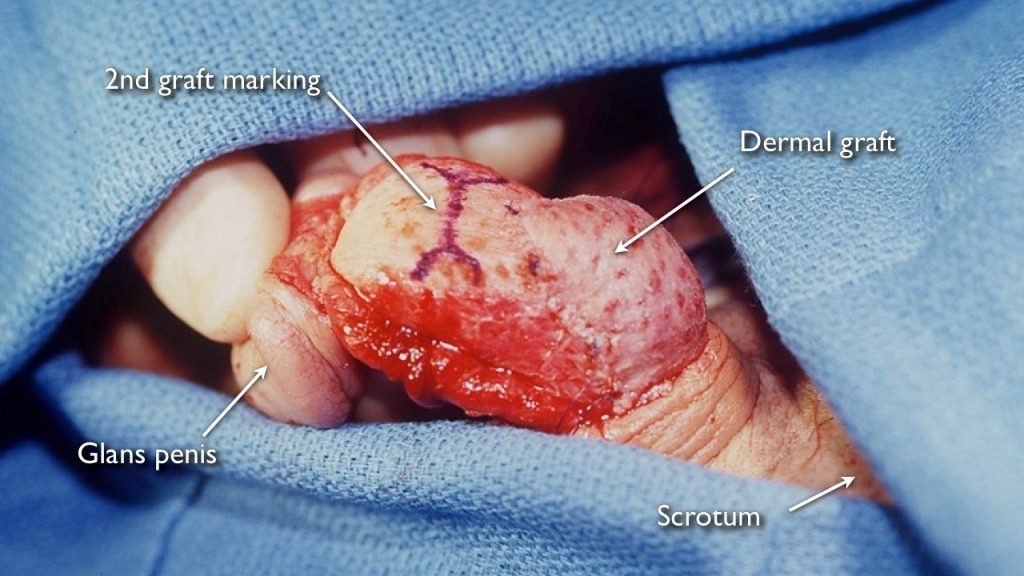
Peyronie’s Disease Graft Surgery
Evaluating Candidates for Peyronie's Disease Surgery
We evaluate the patient’s complete medical history and perform a physical exam and view pictures of the erect penis to determine the best treatment method and if and when surgery may be an appropriate option to fix the Peyronie’s curvature. During this process, we educate our patients so they fully understand the cause of their penile curvature and why they may have pain with erections (if they have painful erections). It is important to discuss the risks and potential benefits of each treatment option, as a patient cannot give proper legal informed consent to treatment without knowing all options.
When a patient has Peyronie’s disease that is in the mature phase and has good erectile function, we ask if the curve interferes with sexual relations. Penile curvature can completely prevent penetration, limit possible sexual positions, or make intercourse uncomfortable for the partner of the patient. These are all valid reasons to pursue a surgical Peyronie’s disease fix. Surgery to straighten a curved penis is generally not considered a cosmetic procedure, so it should be covered by insurance (that does not mean the insurance will pay all costs, but should consider it “medically indicated” and covered based on benefits).
When the curve is mild and not disabling, some patients desire surgery because they find the curvature embarrassing and psychologically troublesome. These patients are advised to weigh the risks vs benefits of surgery. If there is no functional impairment, the patient should carefully consider observation.
Peyronie’s Disease Surgery Results
At the Center for Reconstructive Urology, we have a very high Peyronie’s disease surgery success rate and a very low complication rate. Dr. Gelman is fellowship-trained and expert with over 22 years of experience performing surgery to correct penile curvature, leading to favorable Peyronie’s disease surgery results. Both Peyronie’s disease graft surgery and Peyronie’s disease plication surgery are technically challenging procedures.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}